SIGNAL // LOADING
Loading page

Learn
42 deep reads covering GLP-1 eligibility, testosterone and HRT panels, peptides, NAD, and the lab markers the rest of telehealth skips. Written by the team that reviews your intake.
This is the reference library behind ALUKARD. Every article is written for the person about to type “is my testosterone low” or “is tirzepatide safer than semaglutide” into a search bar at 11pm. We try to answer the question directly in the first paragraph, then unpack the physiology, the labs, the trial data, and the boundary where provider review actually earns its keep.
Articles are medically reviewed and dated. Where we cite trials or guidelines - SURMOUNT-1, STEP-1, ADA 2024 standards of care, AUA testosterone guidance, ESHRE on HRT - they are named, not just gestured at, and collected in the sources list at the foot of each page. If a claim is contested, we say so. If a question doesn’t have a good answer yet, we say that too.
If you want the shorter definitions, visit the glossary. If you want opinionated calls between two options, visit /compare. If you want to start care, the assessment routes you into labs, coaching, or provider review.
Topic cluster
Eligibility, side effects, tirzepatide vs semaglutide, and how to hold the loss once the drug stops.

Most telehealth sites approve nearly every intake that clicks through. We don't. About one in five GLP-1 intakes gets routed elsewhere - thyroid history, pancreatitis, pregnancy plans, or a medication interaction that would put you in the ER. Here's the real criteria before you spend $299 on a service that shouldn't take you.
Read it
They share a class name, not a receptor profile. Tirzepatide delivers ~6 percentage points more average weight loss than semaglutide in pivotal trials. Tolerance, insurance coverage, and state stock often flip the decision anyway. Here's what to weigh before the provider call - and when the right answer is neither.
Read it
Most GLP-1 side effects are titration-related and resolve in 1-2 weeks at each dose step. A small number are red flags that need a same-day call. The difference matters - panic-stopping at week three loses the appetite signal you've been paying for; pushing through actual pancreatitis ends in the ER. Here's how to read the symptom map.
Read it
The 60-80% regain statistic at 12-24 months after stopping GLP-1 isn't a medication failure - it's a foundation failure. Members who built protein, strength, and sleep into the GLP-1 window keep most of the loss. Members who used the medication as a substitute for that work regain almost everything. Here's the maintenance plan that holds.
Read itTopic cluster
Reading a real testosterone panel, who qualifies for TRT, finasteride and DHT trade-offs, and the ratio that actually predicts symptoms.
A single total testosterone number explains almost nothing. A 27-year-old with total T at 650 ng/dL can be symptomatic; a 58-year-old at 420 can feel great. The markers that actually predict how you feel are free testosterone, SHBG, and the metabolic labs most TRT clinics skip. Here's what to look at before anyone prescribes.
Read it
Walk-in low-T clinics approve almost every man who clears the door. We don't. Real TRT eligibility requires two morning labs, a baseline PSA, hematocrit context, fertility planning, and a cardiovascular screen most consumer clinics skip. Here's what gets you through provider review, what flags an automatic decline, and the cases where the right next step isn't testosterone.
Read it
Two men can both have total testosterone at 550 ng/dL. One feels great. The other has the symptoms of a man with total T at 300. The difference is what's bound and what's free - and unless your provider runs SHBG and calculates free T, you're guessing about the number that matters. Here's how the ratio works, why it shifts, and what to do when total looks fine but free isn't.
Read it
Finasteride is the most evidence-backed pharmaceutical option for male pattern hair loss - and it's also the medication that drives the loudest side-effect conversation on the internet. The data behind PSSD (post-finasteride syndrome) deserves an honest read, not a marketing pitch in either direction. Here's the real picture, the alternatives, and the informed-consent standard we hold.
Read itTopic cluster
Where to start when symptoms overlap, the perimenopause panel most GPs won't order, PCOS labs that drive a plan, HRT and ferritin.
"Hormone imbalance" is the most-searched, least-defined term in wellness. Fatigue, weight gain, mood shifts, and low libido can all trace to estrogen, thyroid, testosterone, cortisol, or - most often - ferritin under 50 and six hours of sleep. Here's the structured way to find the real driver instead of throwing $400 at adaptogen blends.
Read it
Perimenopause starts in the late 30s for some women and stretches a decade. Most GPs run a single TSH and FSH and call it inconclusive - because hormones swing day to day in this window, one draw rarely tells the story. Here's the actual panel that maps where you are, when to draw it, and what to do with the result.
Read it
Polycystic ovary syndrome gets diagnosed off symptoms, an ultrasound, or a single elevated testosterone - none of which alone tell a provider what to do. PCOS is a metabolic and hormonal pattern, and the panel that actually moves treatment runs deeper than "borderline polycystic on imaging." Here's what to ask for, and what each marker changes about the plan.
Read it
The 2002 Women's Health Initiative scared a generation of women off hormone therapy. Two decades later, the data has been re-analyzed, the formulations have changed, and the timing window matters more than the original report suggested. Here's where modern HRT actually sits on risk, who benefits most, and what to ask before any prescription.
Read it
A ferritin of 22 ng/mL is technically "in range" at most US labs - and it will leave you exhausted, shedding hair, and unable to tolerate cardio. The reference range was built around "not anemic," not "functionally well." Here's the real ferritin target for women, why it gets missed, and how to fix it without bricking your gut.
Read itTopic cluster
ApoB vs LDL, fasting insulin, HPA axis, biologic age tests, and where NAD+ belongs in a real longevity stack.
Your annual physical reports total cholesterol, HDL, and LDL. None of those numbers actually count the atherogenic particles entering your arteries - ApoB does. Cardiologists shifted to ApoB targeting for primary prevention years ago; primary care is still catching up. Here's why ApoB is the better number, what to target, and how to read discordance with standard lipids.
Read it
By the time HbA1c crosses 5.7% and your PCP calls you "pre-diabetic," your fasting insulin has likely been elevated for 5-10 years. A normal HbA1c is the last metric to change; fasting insulin is one of the first. If you've been told "your blood sugar is fine," run this number before celebrating.
Read it
"Adrenal fatigue" isn't a real diagnosis. The HPA axis - hypothalamus, pituitary, adrenals - is real, measurable, and far more about sleep architecture than about cortisol-support powder. Here's what cortisol patterns actually look like, what to test, and the interventions that reset the axis without supplements.
Read it
Biologic age tests promise a single number that captures "how old your body really is." The science behind them is real - DNA methylation patterns track aging more accurately than the calendar. The clinic interpretations are often oversold. Here's what these tests actually measure, what they're useful for, and the right way to retest.
Read it
NAD+ IV drips sell at $400-800 a session. NMN bottles have become the supplement aisle's hottest trend. Meanwhile, the labs with the strongest longevity evidence - ApoB, HbA1c, fasting insulin - are the ones most "biohackers" never check. Here's the honest read on NAD, and the five labs that actually move the longevity math.
Read itTopic cluster
Where peptides genuinely earn a place in a protocol, where they don't, and when a provider-reviewed plan beats DIY supplementation.
"Peptide therapy" gets sold as anti-aging, muscle-building, sleep-enhancing magic - often for $300-600 a month, shipped from sources that won't even confirm where the molecule was synthesized. Some peptides are FDA-approved breakthroughs. Others are research chemicals repackaged with a wellness aesthetic. Here's the line.
Read it
Every week, someone shows up in our inbox who ordered GLP-1 from an offshore site, spent six months on a "hormone balance" supplement stack, or self-interpreted a ferritin of 18 as "slightly low." The line between smart DIY and expensive self-harm isn't where most people draw it. Here's what to own yourself - and what to stop trying to.
Read itTopic cluster
What a real CMP actually shows and the two supplements with evidence strong enough to move labs on their own.
Your annual physical probably ran a CMP and called the day done. A CMP is 14 markers covering kidney, liver, and electrolyte status - it's wide, but shallow. It will not catch pre-diabetes, insulin resistance, thyroid dysfunction, ApoB, or any hormone issue. Here's what it flags, what it hides, and the four panels you actually need alongside it.
Read it
The supplement aisle sells 200 ingredients. The list with real human evidence and clinically meaningful effect sizes is shorter than five. Here's the honest stack - what to take, what dose, what changes on labs, and what to skip even when the marketing is loud.
Read itMore reads
Not every tired month means TRT. The right call comes from two morning testosterone draws, symptom quality, and the metabolic context that can mimic low T. Here's when treatment is justified, when correction of sleep and insulin resistance should come first, and what monitoring keeps therapy safe.[1]
Read it
Two patients can take the same hormone dose and report opposite outcomes. Estradiol sensitivity is usually a receptor, route, and metabolism story, not a personality story. Here is how clinicians separate true sensitivity from under-dosing, conversion drift, and symptom misattribution.[4]
Read itPlateaus are expected, not proof the medication failed. Most stalls come from adaptation in intake, activity, and sleep long before they come from molecule failure. Here is a practical sequence for troubleshooting plateaus without panic switching.[1][2]
Read itGLP-1 therapy can reduce lean mass if intake and training are neglected. Medication lowers appetite, but it does not protect muscle by default. This guide outlines the minimum protein and resistance-training structure used to preserve lean tissue during active loss.[1][2]
Read it
A thyroid panel is more than TSH. Many persistent fatigue and weight complaints sit in the gap between a normal TSH and poor conversion or autoimmune context. This guide explains what each marker contributes and when follow-up is warranted.[4]
Read itDHEA is often sold as a blanket anti-aging fix, but response depends heavily on baseline hormone context and sex-specific risk. Used selectively, it can help. Used broadly, it can worsen acne, hair issues, and androgen imbalance. Here's how to decide.[4]
Read itCortisol is a rhythm problem as much as a number problem. A single draw can miss the story if morning peak, daytime slope, and evening shutdown are not interpreted together. This article explains common abnormal patterns and what to do next.[5]
Read itLDL-C alone can miss risk. ApoB particle count, triglyceride context, and metabolic markers often explain why two people with similar LDL have different cardiovascular trajectories. Here's how to read the full lipid picture and prioritize interventions.[2]
Read it
Cardiorespiratory fitness is one of the strongest mortality predictors we can measure. VO2max is not just an athlete metric; it is a durable risk marker that can improve with structured aerobic training. Here is what ranges mean and how to improve them.[5]
Read it
Zone 2 is not social-media folklore. It is a sustainable aerobic intensity that improves mitochondrial density, insulin sensitivity, and recovery capacity when done consistently. This guide gives a practical weekly template and progression framework.[5]
Read itMost people track sleep duration but ignore sleep architecture. Time in bed is not the same as restorative sleep. This guide breaks down REM, deep sleep, sleep continuity, and the daily behaviors that improve architecture without overcomplicating your routine.[5]
Read itA1c can look normal while insulin resistance is already progressing. Early markers such as fasting insulin, triglyceride patterns, waist trend, and post-meal response provide earlier warning. This guide explains what to track before prediabetes becomes obvious.[1][2]
Read it
Omega-3 supplementation advice is usually vague. The omega-3 index gives a measurable target and clearer dosing logic than generic fish-oil marketing claims. This article explains target ranges, dosing considerations, and when re-testing matters.[5]
Read it
Vitamin D is important, but it is often overpromised as a cure-all. The real value comes from correcting true deficiency and avoiding excess. This guide reviews 25-OH targets, dosing boundaries, and how vitamin D fits into cardiometabolic strategy.[5]
Read itMagnesium is not one supplement - form determines tolerability and likely use case. Glycinate and threonate are often compared for sleep, stress, and cognitive support. Here's how to choose based on goals and side-effect profile.[5]
Read itCreatine is still underused in women despite strong data on strength, recovery, and healthy aging support. Misconceptions about bloating and hormonal disruption persist. This review explains what studies show and how to dose practically.[5]
Read itMicrobiome content online swings between hype and dismissal. The useful middle ground is linking gut-related symptoms and dietary pattern to measurable metabolic labs. This guide covers where microbiome strategy helps and where labs should lead decisions.[1][2]
Read it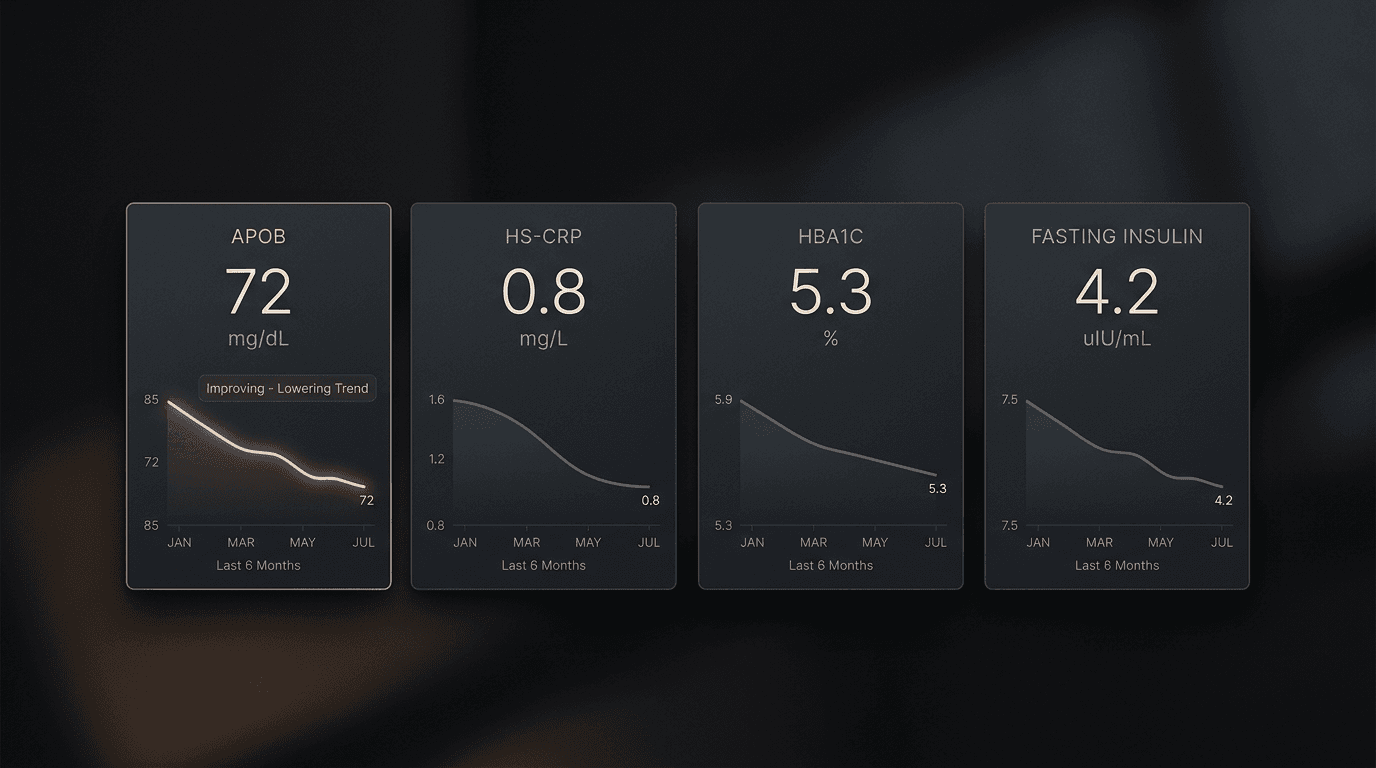
Bone loss is usually silent until fracture. DEXA is one of the few tools that identifies risk early enough to act. This guide explains who should test, how often to recheck, and how to interpret results in practical prevention terms.[4]
Read itMetformin is often framed as a longevity shortcut, but evidence strength differs by population and endpoint. It has a clear role in glycemic management and possible preventive value in selected profiles, but it is not a universal anti-aging default. Here's the balanced evidence read.[2]
Read itRapamycin is one of the most discussed off-label longevity drugs and one of the easiest to misuse. Mechanistic promise is real, but human endpoint evidence is still limited and risk management is non-trivial. This guide covers what is known, unknown, and clinically non-negotiable.[5]
Read it